
Pneumocystis pneumonia (PCP) or pneumocystosis is a form of pneumonia, caused by the yeast-like fungus (which had previously been erroneously classified as a protozoan) Pneumocystis jirovecii.
Pneumocystis is commonly found in the lungs of healthy people, but, being a source of opportunistic infection, it can cause a lung infection in people with a weak immune system. Pneumocystis pneumonia is especially seen in people with cancer undergoing chemotherapy, HIV/AIDS and the use of medications that affect the immune system.
Signs and symptoms

Symptoms of PCP include fever, non-productive cough (because sputum is too viscous to become productive), shortness of breath (especially on exertion), weight loss, and night sweats. There is usually not a large amount of sputum with PCP unless the patient has an additional bacterial infection. The fungus can invade other visceral organs (such as the liver, spleen, and kidney), but only in a minority of cases.
Pneumothorax is a well-known complication of PCP. An acute history of chest pain with breathlessness and diminished breath sounds is typical of pneumothorax.
Disease course
The risk of PCP increases when CD4 positive cell levels are less than 200 cells/μL. In these immunosuppressed individuals the manifestations of the infection are highly variable. The disease attacks the interstitial, fibrous tissue of the lungs, with marked thickening of the alveolar septa and alveoli, leading to significant hypoxia which can be fatal if not treated aggressively. In this situation LDH levels increase and gas exchange is compromised. Oxygen is less able to diffuse into the blood, leading to hypoxia. Hypoxia, along with high arterial carbon dioxide (CO
2) levels, stimulates hyper-ventilatory effort, thereby causing dyspnea (breathlessness).
Diagnosis
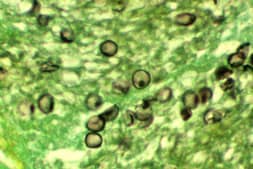
The diagnosis can be confirmed by the characteristic appearance of the chest x-ray, which shows widespread pulmonary infiltrates, and an arterial oxygen level (PaO2) that is strikingly lower than would be expected from symptoms. Gallium 67 scans are also useful in the diagnosis. They are abnormal in approximately 90% of cases and are often positive before the chest x-ray becomes abnormal. The diagnosis can be definitively confirmed by histological identification of the causative organism in sputum or bronchio-alveolar lavage (lung rinse). Staining with toluidine blue, silver stain, periodic-acid schiff stain, or an immunofluorescence assay will show the characteristic cysts. The cysts resemble crushed ping-pong balls and are present in aggregates of 2 to 8 (and not to be confused with Histoplasma or Cryptococcus, which typically do not form aggregates of spores or cells). A lung biopsy would show thickened alveolar septa with fluffy eosinophilic exudate in the alveoli. Both the thickened septa and the fluffy exudate contribute to dysfunctional diffusion capacity which is characteristic of this pneumonia.
Pneumocystis infection can also be diagnosed by immunofluorescent or histochemical staining of the specimen, and more recently by molecular analysis of polymerase chain reaction products comparing DNA samples. Notably, simple molecular detection of Pneumocystis jirovecii in lung fluids does not mean that a person has Pneumocystis pneumonia or infection by HIV. The fungus appears to be present in healthy individuals in the general population.
Prevention and treatment
In immunocompromised patients, prophylaxis with co-trimoxazole (trimethoprim/sulfamethoxazole), atovaquone, or regular pentamidine inhalations may help prevent PCP.
Antipneumocystic medication is used with concomitant steroids in order to avoid inflammation, which causes an exacerbation of symptoms about four days after treatment begins if steroids are not used. By far the most commonly used medication is trimethoprim/sulfamethoxazole, but some patients are unable to tolerate this treatment due to allergies. Other medications that are used, alone or in combination, include pentamidine, trimetrexate, dapsone, atovaquone, primaquine, pafuramidine maleate (under investigation), and clindamycin. Treatment is usually for a period of about 21 days.
Pentamidine is less often used as its major limitation is the high frequency of side effects. These include acute pancreatic inflammation, kidney failure, liver toxicity, decreased white blood cell count, rash, fever, and low blood sugar.
Epidemiology

The disease PCP is relatively rare in people with normal immune systems, but common among people with weakened immune systems, such as premature or severely malnourished children, the elderly, and especially persons living with HIV/AIDS (in whom it is most commonly observed). PCP can also develop in patients who are taking immunosuppressive medications. It can occur in patients who have undergone solid organ transplantation or bone marrow transplantation and after surgery. Infections with Pneumocystis pneumonia are also common in infants with hyper IgM syndrome, an X-linked or autosomal recessive trait.
The causative organism of PCP is distributed worldwide and Pneumocystis pneumonia has been described in all continents except Antarctica. Greater than 75% of children are seropositive by the age of 4, which suggest a high background exposure to the organism. A post-mortem study conducted in Chile of 96 persons who died of unrelated causes (suicide, traffic accidents, and so forth) found that 65 (68%) of them had pneumocystis in their lungs, which suggests that asymptomatic pneumocystis infection is extremely common.
Pneumocystis jirovecii was originally described as a rare cause of pneumonia in neonates. It is commonly believed to be a commensal organism (dependent upon its human host for survival). The possibility of person-to-person transmission has recently gained credence, with supporting evidence coming from many different genotyping studies of Pneumocystis jirovecii isolates from human lung tissue. For example, in one outbreak of 12 cases among transplant patients in Leiden, it was suggested as likely, but not proven, that human-to-human spread may have occurred.
PCP and AIDS
Since the start of the AIDS epidemic, PCP has been closely associated with AIDS. Because it only occurs in an immunocompromised host, it may be the first clue to a new AIDS diagnosis if the patient has no other reason to be immunocompromised (e.g. taking immunosuppressive drugs for organ transplant). An unusual rise in the number of PCP cases in North America, noticed when physicians began requesting large quantities of the rarely used antibiotic pentamidine, was the first clue to the existence of AIDS in the early 1980s.
Prior to the development of more effective treatments, PCP was a common and rapid cause of death in persons living with AIDS. Much of the incidence of PCP has been reduced by instituting a standard practice of using oral co-trimoxazole to prevent the disease in people with CD4 counts less than 200/μL. In populations that do not have access to preventive treatment, PCP continues to be a major cause of death in AIDS.
Nomenclature
The older name Pneumocystis carinii (which now only applies to the Pneumocystis species that is found in rats) is still in common usage. As a result, Pneumocystis pneumonia (PCP) is also known as Pneumocystis jiroveci[i] pneumonia and (incorrectly) as Pneumocystis carinii pneumonia.
Regarding nomenclature, when the name of Pneumocystis pneumonia (PCP) changed from P. carinii pneumonia to P. jirovecii pneumonia, it was at first felt that "PJP" should replace "PCP". However, because the term PCP was already used among physicians that managed patients with Pneumocystis infection, it was rationalized that the term PCP could continue to be used, as it stood for PneumoCystis (jirovecii) Pneumonia.
References
