![]()
Renal cell carcinoma (RCC, also known as hypernephroma, Grawitz tumor, renal adenocarcinoma) is a kidney cancer that originates in the lining of the proximal convoluted tubule, a part of the very small tubes in the kidney that transport waste molecules from the blood to the urine. RCC is the most common type of kidney cancer in adults, responsible for approximately 90-95% of cases. Initial treatment is most commonly either partial or complete removal of the affected kidney(s) and remains the mainstay of curative treatment. Where the cancer has not metastasised (spread to other organs) or burrowed deeper into the tissues of the kidney the 5-year survival rate is 65-90%, but this is lowered considerably when the cancer has spread. It is relatively resistant to radiation therapy and chemotherapy, although some cases respond to targeted therapies such as sunitinib, temsirolimus, bevacizumab, interferon alfa and sorafenib which have improved the outlook for RCC.
The body is remarkably good at hiding the symptoms and as a result people with RCC often have advanced disease by the time it is discovered. The initial symptoms of RCC often include: blood in the urine (occurring in 40% of affected persons at the time they first seek medical attention), flank pain (40%), a mass in the abdomen or flank (25%), weight loss (33%), fever (20%), high blood pressure (20%), night sweats and generally feeling unwell. RCC is also associated with a number of paraneoplastic syndromes (PNS) which are conditions caused by either the hormones produced by the tumour or by the body's attack on the tumour and are present in about 20% of those with RCC. These syndromes most commonly affect tissues which have not been invaded by the cancer. The most common PNSs seen in people with RCC are: anaemia (due to an underproduction of the hormone, erythropoietin), high blood calcium levels, polycythaemia (the opposite to anaemia, due to an overproduction of erythropoietin), thrombocytosis (too many platelets in the blood, leading to an increased tendency for blood clots and bleeds) and secondary amyloidosis. When RCC metastasises it most commonly spreads to the lymph nodes, lungs, liver, adrenal glands, brain or bones.
Signs and symptoms
Historically, medical practitioners expected a person to present with three findings. This classic triad is 1: haematuria, which is when there is blood present in the urine, 2: flank pain, which is pain on the side of the body between the hip and ribs, and 3: an abdominal mass, similar to bloating but larger. It is now known that this classic triad of symptoms only occurs in 10-15% of cases, and is usually indicative that the renal cell carcinoma (RCC) in an advanced stage. Today, RCC is often asymptomatic (meaning little to no symptoms) and is generally detected incidentally when a person is being examined for other ailments.
Other signs and symptom may include haematuria; loin pain; abdominal mass; malaise, which is a general feeling of feeling unwell; weight loss and/or loss of appetite; anaemia resulting from depression of erythropoietin; erythrocytosis (increased production of red blood cells) due to increased erythropoietin secretion; varicocele, which is seen in males as an enlargement of the tissue at the testicle (more often the left testicle) hypertension (high blood pressure) resulting from secretion of renin by the tumour; hypercalcemia, which is elevation of calcium levels in the blood; sleep disturbance or night sweats; recurrent fevers; and chronic fatigue.
Cause

Lifestyle
The greatest risk factors for RCC are lifestyle-related; smoking, obesity and hypertension (high blood pressure) have been estimated to account for up to 50% of cases. Occupational exposure to some chemicals such as asbestos, cadmium, lead, chlorinated solvents, petrochemicals and PAH (polycyclic aromatic hydrocarbon) has been examined by multiple studies with inconclusive results. Another suspected risk factor is the long term use of non-steroidal anti-inflammatory drugs (NSAIDS).
Finally, studies have found that women who have had a hysterectomy are at more than double the risk of developing RCC than those who have not. The reason for this remains unclear.
Genetics
Hereditary factors have a minor impact on individual susceptibility with immediate relatives of people with RCC having a two to fourfold increased risk of developing the condition. Other genetically linked conditions also increase the risk of RCC, including hereditary papillary renal carcinoma, hereditary leiomyomatosis, Birt-Hogg-Dube syndrome, hyperparathyroidism-jaw tumor syndrome, familial papillary thyroid carcinoma, von Hippel-Lindau disease and sickle cell disease.
The most significant disease affecting risk however is not genetically linked â€" patients with acquired cystic disease of the kidney requiring dialysis are 30 times greater more likely than the general population to develop RCC.
Pathophysiology
The tumour arises from the cells of the proximal renal tubular epithelium. It is considered an adenocarcinoma. There are two subtypes: sporadic (that is, non-hereditary) and hereditary. Both such subtypes are associated with mutations in the short-arm of chromosome 3, with the implicated genes being either tumour suppressor genes (VHL and TSC) or oncogenes (like c-Met).
Diagnosis
The first steps taken to diagnose this condition are consideration of the signs and symptoms, and a medical history (the detailed medical review of past health state) to evaluate any risk factors. Based on the symptoms presented, a range of biochemical tests (using blood and/or urine samples) may also be considered as part of the screening process to provide sufficient quantitative analysis of any differences in electrolytes, renal and liver function, and blood clotting times. Upon physical examination, palpation of the abdomen may reveal the presence of a mass or an organ enlargement.
Although this disease lacks characterization in the early stages of tumor development, considerations based on diverse clinical manifestations, as well as resistance to radiation and chemotherapy are important. The main diagnostic tools for detecting renal cell carcinoma are ultrasound, computed tomography (CT) scanning and magnetic resonance imaging (MRI) of the kidneys.
Classification
Renal cell carcinoma (RCC) is not a single entity, but rather a collection of different types of tumours, each derived from the various parts of the nephron (epithelium or renal tubules) and possessing distinct genetic characteristics, histological features, and, to some extent, clinical phenotypes.
Array-based karyotyping can be used to identify characteristic chromosomal aberrations in renal tumors with challenging morphology. Array-based karyotyping performs well on paraffin embedded tumours and is amenable to routine clinical use. See also Virtual Karyotype for CLIA certified laboratories offering array-based karyotyping of solid tumours.
The 2004 World Health Organization (WHO) classification of genitourinary tumours recognizes over 40 subtypes of renal neoplasms. Since the publication of the latest iteration of the WHO classification in 2004, several novel renal tumour subtypes have been described:
- Clear cell papillary renal cell carcinoma and Clear cell renal cell carcinoma with smooth muscle stroma
- Mucinous tubular and spindle cell carcinoma (MTSCC)
- Multilocular cystic clear cell renal cell carcinoma
- Tubulocystic renal cell carcinoma
- Thyroid-like follicular renal cell carcinoma
- Acquired cystic kidney disease-associated renal cell carcinoma
- Renal cell carcinoma with t(6;11) translocation (TFEB)
- Hybrid oncocytoma/chromophobe renal cell carcinoma
- Hereditary leiomyomatosis and renal cell carcinoma(HLRCC)
Laboratory tests
Laboratory tests are generally conducted when the patient presents signs and symptoms that may be characteristic of kidney impairment. They are not primarily used to diagnose kidney cancer, due to its asymptomatic nature and are generally found incidentally during tests for other illnesses such as gallbladder disease. In other words, these cancers are not detected usually because they do not cause pain or discomfort when they are discovered. Laboratory analysis can provide an assessment on the overall health of the patient and can provide information in determining the staging and degree of metastasis to other parts of the body (if a renal lesion has been identified) before treatment is given.
Urine analysis
The presence of blood in urine is a common presumptive sign of renal cell carcinoma. The haemoglobin of the blood causes the urine to be rusty, brown or red in colour. Alternatively, urinalysis can test for sugar, protein and bacteria which can also serve as indicators for cancer. A complete blood cell count can also provide additional information regarding the severity and spreading of the cancer.
Complete blood cell count
The CBC test provides a quantified measure of the different cells in the whole blood sample from the patient. Such cells examined for in this test include red blood cells (erythrocytes), white blood cells (leukocytes) and platelets (thrombocytes). A common sign of renal cell carcinoma is anaemia whereby the patient exhibits deficiency in red blood cells. CBC tests are vital as a screening tool for examination the health of patient prior to surgery. Inconsistencies with platelet counts are also common amongst these cancer patients and further coagulation tests, including Erythrocyte Sedimentation Rate (ESR), Prothrombin Time (PT), Activated Partial Thromboplastin Time (APTT) should be considered.
Blood chemistry
Blood chemistry tests are conducted if renal cell carcinoma is suspected as cancer has the potential to elevate levels of particular chemicals in blood. For example, liver enzymes such as aspartate aminotransferase [AST] and alanine aminotransferase [ALT] are found to be at abnormally high levels. The staging of the cancer can also be determined by abnormal elevated levels of calcium, which suggests that the cancer may have metastasised to the bones. In this case, a doctor should be prompted for a CT scan. Blood chemistry tests also assess the overall function of the kidneys and can allow the doctor to decide upon further radiological tests.
Radiology
The characteristic appearance of renal cell carcinoma (RCC) is a solid renal lesion which disturbs the renal contour. It will frequently have an irregular or lobulated margin and may be seen as a lump on the lower pelvic or abdomen region. Traditionally, 85 to 90% of solid renal masses will turn out to be RCC but cystic renal masses may also be due to RCC. However, the advances of diagnostic modalities are able to incidentally diagnose a great proportion of patients with renal lesions that may appear to be small in size and of benign state. Ten percent of RCC will contain calcifications, and some contain macroscopic fat (likely due to invasion and encasement of the perirenal fat. Deciding on the benign or malignant nature of the renal mass on the basis of its localized size is an issue as renal cell carcinoma may also be cystic. As there are several benign cystic renal lesions (simple renal cyst, haemorrhagic renal cyst, multilocular cystic nephroma, polycystic kidney disease), it may occasionally be difficult for the radiologist to differentiate a benign cystic lesion from a malignant one. The Bosniak classification system for cystic renal lesions classifies them into groups that are benign and those that need surgical resection, based on specific imaging features.
The main imaging tests performed in order to identify renal cell carcinoma are pelvic and abdominal CT scans, ultrasound tests of the kidneys (ultrasonography), MRI scans, intravenous pyelogram (IVP) or renal angiography. Among these main diagnostic tests, other radiologic tests such as excretory urography, positron-emission tomography (PET) scanning, ultrasonography, arteriography, venography, and bone scanning can also used to aid in the evaluation of staging renal masses and to differentiate non-malignant tumours from malignant tumours.
Computed tomography
Contrast-enhanced Computed tomography (CT) scanning is a routinely used imaging procedure in determining the stage of the renal cell carcinoma in the abdominal and pelvic regions of the patient. CT scans have the potential to distinguish solid masses from cystic masses and may provide information on the localization, stage or spread of the cancer to other organs of the patient. Key parts of the human body which are examined for metastatic involvement of renal cell carcinoma may include the renal vein, lymph node and the involvement of the inferior vena cava. According to a study conducted by Sauk et al., multidetector CT imaging characteristics have applications in diagnosing patients with clear renal cell carcinoma by depicting the differences of these cells at the cytogenic level.
Ultrasound
Ultrasonographic examination can be useful in evaluating questionable asymptomatic kidney tumours and cystic renal lesions if Computed Tomography imaging is inconclusive. This safe and non-invasive radiologic procedure uses high frequency sound waves to generate an interior image of the body on a computer monitor. The image generated by the ultrasound can help diagnose renal cell carcinoma based on the differences of sound reflections on the surface of organs and the abnormal tissue masses. Essentially, ultrasound tests can determine whether the composition of the kidney mass is mainly solid or filled with fluid.
A Percutaneous biopsy can be performed by a radiologist using ultrasound or computed tomography to guide sampling of the tumour for the purpose of diagnosis by pathology. However this is not routinely performed because when the typical imaging features of renal cell carcinoma are present, the possibility of an incorrectly negative result together with the risk of a medical complication to the patient may make it unfavourable from a risk-benefit perspective. However, biopsy tests for molecular analysis to distinguish benign from malignant renal tumours is of investigative interest.
Magnetic resonance imaging
Magnetic Resonance Imaging (MRI) scans provide an image of the soft tissues in the body using radio waves and strong magnets. MRI can be used instead of CT if the patient exhibits an allergy to the contrast media administered for the test. Sometimes prior to the MRI scan, an intravenous injection of a contrasting material called gadolinium is given to allow for a more detailed image. Patients on dialysis or those who have renal insufficiency should avoid this contrasting material as it may induce a rare, yet severe, side effect known as nephrogenic systemic fibrosis. A bone scan or brain imaging is not routinely performed unless signs or symptoms suggest potential metastatic involvement of these areas. MRI scans should also be considered to evaluate tumour extension which has grown in major blood vessels, including the vena cava, in the abdomen. MRI can be used to observe the possible spread of cancer to the brain or spinal cord should the patient present symptoms that suggest this might be the case.
Intravenous pyelogram
Intravenous pyelogram (IVP) is a useful procedure in detecting the presence of abnormal renal mass in the urinary tract. This procedure involves the injection of a contrasting dye into the arm of the patient. The dye travels from the blood stream and into the kidneys which in time, passes into the kidneys and bladder. This test is not necessary if a CT or MRI scan has been conducted.
Renal angiography
Renal angiography uses the same principle as IVP, as this type of X-ray also uses a contrasting dye. This radiologic test is important in diagnosing renal cell carcinoma as an aid for examining blood vessels in the kidneys. This diagnostic test relies on the contrasting agent which is injected in the renal artery to be absorbed by the cancerous cells. The contrasting dye provides a clearer outline of abnormally-oriented blood vessels believed to be involved with the tumour. This is imperative for surgeons as it allows the patient’s blood vessels to be mapped prior to operation.
Staging
The staging of renal cell carcinoma is the most important factor in predicting its prognosis. Staging can follow the TNM staging system, where the size and extent of the tumour (T), involvement of lymph nodes (N) and metastases (M) are classified separately. Also, it can use overall stage grouping into stage I-IV, with the 1997 revision of AJCC described below:
At diagnosis, 30% of renal cell carcinomas have spread to the ipsilateral renal vein, and 5-10% have continued into the inferior vena cava.
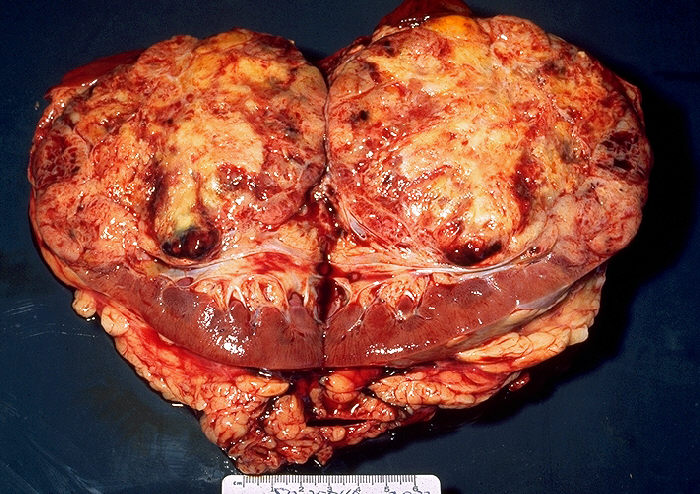
Histopathology
The gross and microscopic appearance of renal cell carcinomas is highly variable. The renal cell carcinoma may present reddened areas where blood vessels have bled, and cysts containing watery fluids. The body of the tumour shows large blood vessels that have walls composed of cancerous cells. Gross examination often shows a yellowish, multilobulated tumor in the renal cortex, which frequently contains zones of necrosis, haemorrhage and scarring. In a microscopic context, there are four major histologic subtypes of renal cell cancer: clear cell (conventional RCC, 75%), papillary (15%), chromophobic (5%), and collecting duct (2%). Sarcomatoid changes (morphology and patterns of IHC that mimic sarcoma, spindle cells) can be observed within any RCC subtype and are associated with more aggressive clinical course and worse prognosis. Under light microscopy, these tumour cells can exhibit papillae, tubules or nests, and are quite large, atypical, and polygonal.
Recent studies have brought attention to the close association of the type of cancerous cells to the aggressiveness of the condition. Some studies suggest that these cancerous cells accumulate glycogen and lipids, their cytoplasm appear "clear", the nuclei remain in the middle of the cells, and the cellular membrane is evident. Some cells may be smaller, with eosinophilic cytoplasm, resembling normal tubular cells. The stroma is reduced, but well vascularised. The tumour compresses the surrounding parenchyma, producing a pseudocapsule.
The most common cell type exhibited by renal cell carcinoma is the clear cell, which is named by the dissolving of the cells' high lipid content in the cytoplasm. The clear cells are thought to be the least likely to spread and usually respond more favourably to treatment. However, most of the tumours contain a mixture of cells. The most aggressive stage of renal cancer is believed to be the one in which the tumour is mixed, containing both clear and granular cells.
The recommended histologic grading schema for RCC is the Fuhrman system (1982), which is an assessment based on the microscopic morphology of a neoplasm with haematoxylin and eosin (H&E staining). This system categorises renal cell carcinoma with grades 1, 2, 3, 4 based on nuclear characteristics. The details of the Fuhrman grading system for RCC are shown below:
Nuclear grade is believed to be one of the most imperative prognostic factors in patients with renal cell carcinoma. However, a study by Delahunt et al. (2007) has shown that the Fuhrman grading is ideal for clear cell carcinoma but may not be appropriate for chromophobe renal cell carcinomas and that the staging of cancer (accomplished by CT scan) is a more favourable predictor of the prognosis of this disease. In relation to renal cancer staging, the Heidelberg classification system of renal tumours was introduced in 1976 as a means of more completely correlating the histopathological features with the identified genetic defects.
Prognosis
The prognosis for renal cell carcinoma is largely influenced by a variety of factors, including tumour size, degree of invasion and metastasis, histologic type, and nuclear grade. For metastatic renal cell carcinoma, factors which may present a poor prognosis include a low Karnofsky performance-status score (a standard way of measuring functional impairment in patients with cancer), a low haemoglobin level, a high level of serum lactate dehydrogenase, and a high corrected level of serum calcium. For non-metastatic cases, the Leibovich scoring algorithm may be used to predict post-operative disease progression.
Renal cell carcinoma is one of the cancers most strongly associated with paraneoplastic syndromes, most often due to ectopic hormone production by the tumour. The treatment for these complications of RCC is generally limited beyond treating the underlying cancer.
For those that have tumour recurrence after surgery, the prognosis is generally poor. Renal cell carcinoma does not generally respond to chemotherapy or radiation. Immunotherapy, which attempts to induce the body to attack the remaining cancer cells, has shown promise. Recent trials are testing newer agents, though the current complete remission rate with these approaches is still low, around 12-20% in most series. Most recently, treatment with tyrosine kinase inhibitors including nexavar, pazopanib, and rapamycin have shown promise in improving the prognosis for advanced RCC.
Management

The type of treatment depends on multiple factors and the individual, some of which include:
- Stage of renal cell carcinoma
- Organs and parts of the body affected/unaffected
- Type of renal cell carcinoma
- Pre-existing or comorbid conditions
- Overall health and age of the person
Every form of treatment has both risks and benefits; a health care professional will provide the best options that suit the individual circumstances.
Active surveillance
Active surveillance or "watchful waiting" is becoming more common as small renal masses or tumours are being detected and also within the older generation when surgery is not always suitable. Active surveillance involves completing various diagnostic procedures, tests and imaging to monitor the progression of the RCC before embarking on a more high risk treatment option like surgery. In the elderly, patients with co-morbidities, and in poor surgical candidates, this is especially useful.
Surgery
Different procedures may be most appropriate, depending on circumstances.
Radical nephrectomy is the removal of the entire affected kidney including Gerota's fascia, the adrenal gland which is on the same side as the affected kidney, and the regional lymph nodes, all at the same time. This method, although severe, is effective. But it is not always appropriate, as it is a major surgery that contains the risk of complication both during and after the surgery and can have a longer recovery time. It is important to note that the other kidney must be fully functional, and this technique is most often used when there is a large tumour present in only one kidney.
Nephron-sparing partial nephrectomy is used when the tumor is small (less than 4Â cm in diameter) or when the patient has other medical concerns such as diabetes or hypertension. The partial nephrectomy involves the removal of the affected tissue only, sparing the rest of the kidney, Gerota's fascia and the regional lymph nodes. This allows for more renal preservation as compared to the radical nephrectomy, and this can have positive long term health benefits. Larger and more complex tumors can also be treated with partial nephrectomy by surgeons with a lot of kidney surgery experience.
Laparoscopic nephrectomy uses laparoscopic surgery, with minimally invasive surgical techniques. Commonly referred to as key hole surgery, this surgery does not have the large incisions seen in a classically performed radical or partial nephrectomy, but still successfully removes either all or part of the kidney. Laparoscopic surgery is associated with shorter stays in the hospital and quicker recovery time but there are still risks associated with the surgical procedure.
Surgery for metastatic disease: If metastatic disease is present surgical treatment may still a viable option. Radical and partial nephrectomy can still occur, and in some cases if the metastasis is small this can also be surgically removed. This depends on what stage of growth and how far the disease has spread.
Targeted ablative therapies
Targeted ablative therapies are also known as percutaneous ablative therapies. Although the use of laparoscopic surgical techniques for complete nephrectomies has reduced some of the risks associated with surgery, surgery of any sort in some cases will still not be feasible. For example, the elderly, people already suffering from severe renal dysfunction, or people who have several comorbidities, surgery of any sort is not warranted. Instead there are targeted therapies which do not involve the removal of any organs or serious surgery. Rather, these therapies involve the ablation of the tumor or the affected area. Ablative treatments use imaging such as computed tomography (CT) or magnetic resonance imaging (MRI) to identify the location of the tumors, which ideally are smaller than 3.5Â cm and to guide the treatment. However there are some cases where ablation can be used on tumors that are larger.
The two main types of ablation techniques that are used for renal cell carcinoma are radio frequency ablation and cryoablation.
Radio frequency ablation uses an electrode probe which is inserted into the affected tissue, to send radio frequencies to the tissue to generate heat through the friction of water molecules. The heat destroys the tumor tissue. Cell death will generally occur within minutes of being exposed to temperatures above 50 °C.
Cryoablation also involves the insertion of a probe into the affected area, however, cold is used to kill the tumor instead of heat. The probe is cooled with chemical fluids which are very cold. The freezing temperatures cause the tumor cells to die by causing osmotic dehydration, which pulls the water out of the cell destroying the enzyme, organelles, cell membrane and freezing the cytoplasm.
Targeted drug treatments
Immunotherapy is a method that activates the person's immune system and uses it to their own advantage. It was developed after observing that in some cases there was spontaneous regression. That is, the renal cell carcinoma improved with no other therapies. Immunotherapy capitalises on this phenomenon and aims to build up a person's immune response to cancer cells. Other medications target things such as growth factors that have been shown to promote the growth and spread of tumours. They inhibit the growth factor in order to prevent tumours from forming. There have been many different medications developed and most have only been approved in the last seven or so years.
Some of the most recently developed treatments are listed below:
Each of the treatments listed above is slightly different; some only work for a little while and others need to be used in conjunction with other therapies. There are also different side effects and risks associated with different forms of medication. As always, the advice of a health care professional should be sought if considering any of the therapies mentioned.
Chemotherapy
Chemotherapy and radiotherapy are not as successful in the case of RCC. RCC is resistant in most cases but there is about a 4-5% success rate sometimes, but this is often short lived with more tumours and growths developing later.
Vaccine
Cancer vaccines are being developed but so far have been found to be effective for only certain forms of the RCC. The vaccines are being designed to "prime" the immune system to provide tumour specific immunity. They are still being developed but the present another treatment possibility.
Adjuvant and neoadjuvant therapy
Adjuvant therapy, which refers to therapy given after a primary surgery, has not been found to be beneficial in renal cell cancer. Conversely, neoadjuvant therapy is administered before the intended primary or main treatment. In some cases neoadjuvant therapy has been shown to decrease the size and stage of the RCC to then allow it to be surgically removed. This is a new form of treatment and the effectiveness of this approach is still being assessed in clinical trials.
Metastatic renal cell carcinoma
.jpg)
Metastatic renal cell carcinoma (mRCC) is the spread of the primary renal cell carcinoma from the kidney to other organs. 25-30% of people have this metastatic spread by the time they are diagnosed with renal cell carcinoma. This high proportion is explained by the fact that clinical signs are generally mild until the disease progresses to a more severe state. The most common sites for metastasis are the lymph nodes, lung, bones, liver and brain. How this spread affects the staging of the disease and hence prognosis is discussed in the “Diagnosis†and “Prognosis†section.
MRCC has a poor prognosis compared to other cancers although average survival times have increased in the last few years due to treatment advances. Average survival time in 2008 for the metastatic form of the disease was under a year and by 2013 this improved to an average of 22 months. Despite this improvement the 5 year survival rate for mRCC remains under 10% and 20-25% of suffers remain unresponsive to all treatments and in these cases, the disease has a rapid progression.
The available treatments for RCC discussed in the “Treatment†section are also relevant for the metastatic form of the disease. Options include interleukin-2 which is a standard therapy for advanced renal cell carcinoma. In the past six years, seven new treatments have been approved specifically for mRCC (sunitinib, temsirolimus, bevacizumab, sorafenib, everolimus, pazopanib and axitinib). These new treatments are based on the fact that renal cell carcinomas are very vascular tumors â€" they contain a large number of blood vessels. The drugs aim to inhibit the growth of new blood vessels in the tumors, hence slowing growth and in some cases reducing the size of the tumors. Side effects unfortunately are quite common with these treatments and include:
- Gastrointestinal effects - nausea, vomiting, diarrhea, anorexia
- Respiratory effects - coughing, dyspnea (difficulty breathing)
- Cardiovascular effects -hypertension(high blood pressure)
- Neurological effects - intracranial hemorrhage (bleeding into the brain), thrombosis (blood clots) in the brain
- Effects on the skin and mucus membranes - rashes, hand-foot syndrome, stomatitis
- Bone marrow suppression -resulting in reduced white blood cells, increasing the risk of infections plus anemia and reduced platelets
- Renal effects - impaired kidney function
- Fatigue.
Radiotherapy and chemotherapy are more commonly used in the metastatic form of RCC to target the secondary tumors in the bones, liver, brain and other organs. While not curative, these treatments do provide relief for suffers from symptoms associated with the spread of tumors. Other potential treatments are still being developed, including tumor vaccines and small molecule inhibitors.
Epidemiology
The incidence of the disease varies according to geographic, demographic and, to a lesser extent, hereditary factors. There are some known risk factors, however the significance of other potential risk factors remains more controversial. The incidence of the cancer has been increasing in frequency worldwide at a rate of approximately 2-3% per decade until the last few years where the number of new cases has stabilised.
The incidence of RCC varies between sexes, ages, races and geographic location around the world. Men have a higher incidence than women (approximately 1.6:1) and the vast majority are diagnosed after 65 years of age. Asians reportedly have a significantly lower incidence of RCC than whites and while African countries have the lowest reported incidences, African Americans have the highest incidence of the population in the United States. Developed countries have a higher incidence than developing countries, with the highest rates found in North America, Europe and Australia / New Zealand
History
.jpg/800px-Metastatic_renal_cell_carcinoma,_intrabronchial_(7425443104).jpg)
Daniel Sennert made the first reference suggesting a tumour arising in the kidney in his text Practicae Medicinae, first published in 1613.
Miril published the earliest unequivocal case of renal carcinoma in 1810. He described the case of Françoise Levelly, a 35 year old woman, who presented to Brest Civic Hospital on April 6, 1809, supposedly in the late stages of pregnancy.
Koenig published the first classification of renal tumours based on macroscopic morphology in 1826. Koenig divided the tumors into scirrhous, steatomatous, fungoid and medullary forms.
Hypernephroma controversy
Following the classification of the tumour, researchers attempted to identify the tissue of origin for renal carcinoma.
The pathogenesis of renal epithelial tumours was debated for decades. The debate was initiated by Paul Grawitz when in 1883, he published his observations on the morphology of small, yellow renal tumours. Grawitz concluded that only alveolar tumours were of adrenal origin, whereas papillary tumours were derived from renal tissue.
In 1893, Paul Sudeck challenged the theory postulated by Grawitz by publishing descriptions of renal tumours in which he identified atypical features within renal tubules and noted a gradation of these atypical features between the tubules and neighboring malignant tumour. In 1894, Otto Lubarsch, who supported the theory postulated by Grawitz coined the term hypernephroid tumor, which was amended tohypernephroma by Felix Victor Birch-Hirschfeld to describe these tumours.
Vigorous criticism of Grawitz was provided by Oskar Stoerk in 1908, who considered the adrenal origin of renal tumours to be unproved. Despite the compelling arguments against the theory postulated by Grawitz, the term hypernephroma, with its associated adrenal connotation, persisted in the literature.
Foot and Humphreys, and Foote et al. introduced the term Renal Celled Carcinoma to emphasize a renal tubular origin for these tumours. Their designation was slightly altered by Fetter to the now widely accepted term Renal Cell Carcinoma.
Convincing evidence to settle the debate was offered by Oberling et al. in 1959 who studied the ultrastructure of clear cells from eight renal carcinomas. They found that the tumour cell cytoplasm contained numerous mitochondria and deposits of glycogen and fat. They identified cytoplasmic membranes inserted perpendicularly onto basement membrane with occasional cells containing microvilli along the free borders. They concluded that these features indicated that the tumours arose from the epithelial cells of the renal convoluted tubule, thus finally settling one of the most debated issues in tumour pathology.
