
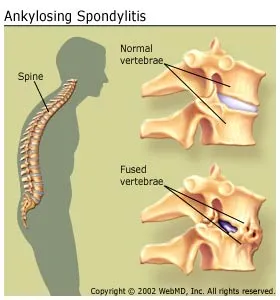
Ankylosing spondylitis (AS, from Greek ankylos, fused; spondylos, vertebra; -itis, inflammation), previously known as Bechterew's disease (or syndrome) and Marie-Strümpell disease, is a chronic inflammatory disease of the axial skeleton, with variable involvement of peripheral joints and nonarticular structures. AS is a member of the group of the spondyloarthropathies, with a strong genetic predisposition. It mainly affects joints in the spine and the sacroiliac joint in the pelvis. In severe cases, it can eventually cause complete fusion and rigidity of the spine.
"Bamboo spine" develops when the outer fibers of the fibrous ring of the intervertebral disks ossify, which results in the formation of marginal syndesmophytes between adjoining vertebrae.
It usually begins in the second or third decade of life and tends to occur more often in males.
Signs and symptoms

- Symptoms appear gradually, most commonly between 15 and 45 years of age.
- Sacroiliitis is usually one of the earliest manifestation of AS. The initial symptom is usually a typical chronic dull pain, insidious in onset, felt deep in the lower lumbar or gluteal region, accompanied by low-back morning stiffness. It can occur in in the middle part of the spine or the entire spine, often with pain referred to one or the other buttock or the back of the thigh from the sacroiliac joint.
- Pain is often severe at rest, but improves with physical activity. However, many experience inflammation and pain to varying degrees regardless of rest and movement.
- Enthesopathy: Ankylosing spondylitis is one of a cluster of conditions known as seronegative spondyloarthropathies, in which rheumatoid factor tests are negative and the characteristic pathological lesion is an inflammation of the enthesis (the insertion of tensile connective tissue into bone).
- Since the initial signs and symptoms are not specific for ankylosing spondylitis, there is a lag-time between onset of disease and diagnosis, which averages between 8.5 years and 11.4 years.
- Arthritis in the hips and shoulders may occur.
- The most common extraarticular manifestation is acute anterior uveitis which can antedate the spondylitis. About 40 percent of AS patients experience inflammation in the anterior chamber of the eye (uveitis), causing redness, eye pain, floaters and photophobia. Visual acuity is usually maintained and the fundus is normal. This is thought to be due to the association that both AS and uveitis have with the inheritance of the HLA-B27 antigen.
- Loss of spinal mobility, with limitation of anterior flexion, lateral flexion, and extension of the lumbar spine, is seen.
- Lung involvement, is characterized by slowly progressive fibrosis of the upper portion of the lung. There is limitation of chest expansion. Recurrent chest infection is the most common cause of death.
- Aortitis, aortic valve insufficiency or cardiac conduction disturbances.
- Prostatitis occurs with increased frequency in men.
- The most serious complication of the spinal disease is spinal fracture, which can occur with even minor trauma to the rigid, osteoporotic spine.
- Mortality attributable to AS is largely the result of spinal trauma, aortic insufficiency, respiratory failure, amyloid nephropathy, or complications of therapy such as upper gastrointestinal hemorrhage.
- Other common symptoms of AS include: chest pain and generalized fatigue. Less commonly ectasia of the sacral nerve root sheaths may occur.
- When the condition presents before the age of 18, it is relatively likely to cause pain and swelling of large limb joints, particularly the knee, Also pain in the groin not associated with UTI (urinary tract infection). In prepubescent cases, pain and swelling may also manifest in the ankles and feet, where heel spurs may also develop.
Pathophysiology
Ankylosing spondylitis (AS) is a systemic rheumatic disease, meaning it affects the entire body. Approximately 90% of AS patients express the HLA-B27 genotype, meaning there is a strong genetic association. 1-2% of individuals with the HLA-B27 genotype contract the disease. Tumor necrosis factor-alpha (TNF α) and IL-1 are also implicated in ankylosing spondylitis. Autoantibodies specific for AS have not been identified. Anti-neutrophil cytoplasmic antibodies (ANCAs) are associated with AS, but do not correlate with disease severity. In a study of 40 patients with AS, ANCA was an infrequent finding, being present in six patients.
The association of AS with HLA-B27 suggests the condition involves CD8 T cells, which interact with HLA-B. This interaction is not proven to involve a self antigen, and at least in the related Reiter's syndrome (reactive arthritis), which follows infections, the antigens involved are likely to be derived from intracellular microorganisms. There is, however, a possibility that CD4 T cells are involved in an aberrant way, since HLA-B27 appears to have a number of unusual properties, including possibly an ability to interact with T cell receptors in association with CD4 (usually cytotoxic T lymphocytes with CD8 react with HLAB antigen as it is a MHC class 1 antigen).
In 2001, it was suggested that AS arises from a cross-reaction between HLA-B27 and antigens of the Klebsiella bacterial genus. There is evidence such cross reactivity with B27 as well as collagen fibers I,III, and IV in those patients suffering from AS. Some authorities argue that the elimination of the prime nutrients of Klebsiella (i.e. starches) would decrease antigenemia and improve the musculoskeletal symptoms. However, as Khan (2002) argues, evidence for a correlation between Klebsiella and AS is circumstantial so far, and the efficacy of low-starch diets has not yet been scientifically evaluated. A randomized controlled trial in Turkey demonstrated that 12-week therapy with moxifloxacin (which would kill Klebsiella) resulted in "significant and sustained improvement" in inflammatory symptoms in patients with ankylosing spondylitis.
Toivanen (1999) found no support for the role of Klebsiella in the etiology of primary AS.
Diagnosis
_anagoria.JPG/230px-0510_Spondylitis_ankylosans_(morbus_bechterew)_anagoria.JPG)
There is no direct test to diagnose AS. The Schober's test is a useful clinical measure of flexion of the lumbar spine performed during the physical examination.Magnetic resonance imaging (MRI), and X-ray studies of the spine, which show characteristic spinal changes and sacroiliitis, combined with a genetic marker blood test are the major diagnostic tools.
Radiographic features
- The earliest changes in the sacroiliac joints demonstrable by plain xâ€"ray shows erosions and sclerosis.
- Progression of the erosions leads to pseudo widening of the joint space and bony ankylosis.
- X-ray spine can reveal bamboo spine appearance.
- A drawback of X-ray diagnosis is the signs and symptoms of AS have usually been established as long as 8â€"10 years prior to X-ray-evident changes occurring on a plain film X-ray, which means a delay of as long as 10 years before adequate therapies can be introduced. Options for earlier diagnosis are tomography and MRI of the sacroiliac joints, but the reliability of these tests is still unclear.
Blood parameters
During acute inflammatory periods, AS patients will sometimes show an increase in the blood concentration of C-reactive protein (CRP) and an increase in the erythrocyte sedimentation rate (ESR), but there are many with AS whose CRP and ESR rates do not increase, so normal CRP and ESR results do not always correspond with the amount of inflammation that is actually present. In other words, some people with AS have normal levels of CRP and ESR, despite experiencing a significant amount of inflammation in their bodies.
Genetic testing
Variations of the HLA-B gene increase the risk of developing ankylosing spondylitis, although it is not a diagnostic test. Those with the HLA-B27 variant are at a higher risk than the general population of developing the disorder. HLA-B27, demonstrated in a blood test, can occasionally help with diagnosis, but in itself is not diagnostic of AS in a person with back pain. Over 95% of people that have been diagnosed with AS are HLA-B27 positive, although this ratio varies from population to population (about 50% of African American patients with AS possess HLA-B27, and it is close to 80% among AS patients from Mediterranean countries). In early onset disease HLA-B7/B*2705 heterozygotes exhibited the highest risk for disease.
BASDAI
The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), developed in Bath (UK), is an index designed to detect the inflammatory burden of active disease. The BASDAI can help to establish a diagnosis of AS in the presence of other factors such as HLA-B27 positivity, persistent buttock pain which resolves with exercise, and X-ray or MRI evident involvement of the sacroiliac joints. (See: "Diagnostic Tools", below) It can be easily calculated and accurately assesses a patient's need for additional therapy; a patient with a score of four out of a possible 10 points while on adequate NSAID therapy is usually considered a good candidate for biologic therapy.
The Bath Ankylosing Spondylitis Functional Index (BASFI) is a functional index which can accurately assess a patient's functional impairment due to the disease, as well as improvements following therapy. (See: "Diagnostic Tools", below) The BASFI is not usually used as a diagnostic tool, but rather as a tool to establish a patient's current baseline and subsequent response to therapy.
Treatment

There is no cure for AS, although treatments and medications can reduce symptoms and pain.
Medication
The major types of medications used to treat ankylosing spondylitis are pain-relievers and drugs aimed at stopping or slowing the progression of the disease. Pain-relieving drugs come in two major classes:
- The mainstay of therapy in all seronegative spondyloarthropathies are anti-inflammatory drugs, which include NSAIDs such as ibuprofen, phenylbutazone, diclofenac, indomethacin, naproxen and COX-2 inhibitors, which reduce inflammation and pain. Indomethacin is a drug of choice. 2012 research showed that patients with elevated acute phase reactants seem to benefit most from continuous treatment with NSAIDs.
- Opioid analgesics
Drugs used to treat the progression of the disease include:
- Disease-modifying antirheumatic drugs (DMARDs) such as sulfasalazine can be used in patients with peripheral arthritis. For axial involvement, sulfasalazine is less effective. Other DMARDS, such as methotrexate did not have enough evidence to prove their effect. Generally, systemic corticosteroids were not used due to lack of evidence. Local injection with corticosteroid can be used for selected patients with peripheral arthritis.
- Tumor necrosis factor-alpha (TNFα) blockers (antagonists), such as the biologics etanercept (Enbrel), infliximab (Remicade), golimumab (Simponi) and adalimumab (Humira), have shown good short-term effectiveness in the form of profound and sustained reduction in all clinical and laboratory measures of disease activity. Trials are ongoing to determine their long-term effectiveness and safety.> The major drawback is the cost.
- Anti-interleukin-6 inhibitors such as Tocilizumab, currently approved for the treatment of rheumatoid arthritis, and rituximab, a monoclonal antibody against CD20, are also undergoing trials.
Surgery
In severe cases of AS, surgery can be an option in the form of joint replacements, particularly in the knees and hips. Surgical correction is also possible for those with severe flexion deformities (severe downward curvature) of the spine, particularly in the neck, although this procedure is considered very risky.
In addition, AS can have some manifestations which make anaesthesia more complex. Changes in the upper airway can lead to difficulties in intubating the airway, spinal and epidural anaesthesia may be difficult owing to calcification of ligaments, and a small number of patients have aortic insufficiency. The stiffness of the thoracic ribs results in ventilation being mainly diaphragm-driven, so there may also be a decrease in pulmonary function.
Physical therapy
Though physical therapy remedies have been scarcely documented, some therapeutic exercises are used to help manage lower back, neck, knee, and shoulder pain. Some therapeutic exercises include:
- Low intensity aerobic exercise
- Transcutaneous electrical nerve stimulation (TENS)
- Thermotherapy
- Proprioceptive neuromuscular facilitation (PNF)
- Exercise programs, either at home or supervised, are better than not having an exercise program;
- Group exercises are better than home exercises;
- Extending regular group exercises with few weeks exercising at a spa resort is better than group exercises alone.
Low intensity aerobic exercises have shown to have profound positive effects regarding pulmonary function, quality of life, and functional capacity.
Spa treatments utilizing thermal baths coupled with tumor necrosis factor inhibitors (TNF) have shown a long-term improvement in AS patients. Spa treatments coupled with TNF inhibitors have no disease relapse among AS patients.
Moderate-to-high impact exercises like jogging are generally not recommended or recommended with restrictions due to the jarring of affected vertebrae that can worsen pain and stiffness in some patients.
Prognosis

Prognosis is related to disease severity. AS can range from mild to progressively debilitating and from medically controlled to refractory. Some cases may have times of active inflammation followed by times of remission resulting in minimal disability, while others never have times of remission and have acute inflammation and pain, leading to significant disability. Complete fusion of the spine can lead to a reduced range of motion and increased pain, as well as total joint destruction which could lead to a joint replacement.
Over a long-term period, osteopenia or osteoporosis of the AP spine may occur, causing eventual compression fractures and a back "hump". Typical signs of progressed AS are the visible formation of syndesmophytes on X-rays and abnormal bone outgrowths similar to osteophytes affecting the spine. The fusion of the vertebrae paresthesia is a complication due to the inflammation of the tissue surrounding nerves.
Organs commonly affected by AS, other than the axial spine and other joints, are the heart, lungs, eyes, colon, and kidneys. Other complications are aortic regurgitation, Achilles tendinitis, AV node block and amyloidosis. Owing to lung fibrosis, chest X-rays may show apical fibrosis, while pulmonary function testing may reveal a restrictive lung defect. Very rare complications involve neurologic conditions such as the cauda equina syndrome.
Mortality
Mortality is increased in patients with AS and circulatory disease is the most frequent cause of death; and because increased mortality in ankylosing spondylitis is related to disease severity, factors negatively affecting patient outcome include:
- Male gender
- Plus 3 of the following in the first 2 years of disease:
- Erythrocyte sedimentation rate (ESR) >30Â mm/h
- Unresponsive to NSAIDs
- Limitation of lumbar spine
- Sausage-like fingers or toes
- Oligoarthritis
- Onset <16 years old
Effect on gait
The hunched position that often results from complete spinal fusion can have an effect on a person’s gait. Increased spinal kyphosis will lead to a forward and downward shift in center of mass (COM). This shift in COM has been shown to be compensated by increased knee flexion and ankle plantarflexion. The gait of someone with ankylosing spondylitis often has a cautious pattern because they have decreased ability to absorb shock, and they cannot see the horizon.
Research
In 2007, a collaborative effort by an international team of researchers in the United Kingdom, Australia and the United States led to the discovery of two genes that also contribute to the cause of AS: ARTS-1 and IL23R. The findings were published in the November 2007 edition of Nature Genetics, a journal that emphasizes research on the genetic basis for common and complex diseases. Together with HLA-B27, these two genes account for roughly 70 percent of the overall incidence of the disease.
Epidemiology
The overall prevalence of AS is between 0.1 and 0.2 percent of the general population. The disease is most prevalent in Northern European countries, and seen least in people of Afro-Caribbean descent. It is more commonly diagnosed in men, with two males being diagnosed for every one female though the sex differences may be higher in some populations. Many rheumatologists believe the number of women with AS is underdiagnosed, as most women tend to experience milder cases of the disease. AS symptoms may also present differently in woman. Men usually have their spine and hips affected, whereas women may present in whole MSK. Fingers, toes, ribcage,all over. The majority of AS patients, including 95 percent of white patients, express the HLA-B27 antigen and high levels of immunoglobulin A (IgA) in the blood. The onset of the disease is typically between 15 and 25 years of age.
Risk factors for ankylosing spondylitis are a family history of spondyloarthritis, the presence of the antigen HLA-B27. in the body, as well as various environmental factors. One's risk of developing the disease increases by 16% when they have one or more of these factors. As the disease progresses, it can cause the vertebrae and the lumbosacral joint to ossify, resulting in the fusion of the spine. This places the spine in a vulnerable state because it becomes one bone, which causes it to lose its range of motion as well as putting it at risk for spinal fractures. This not only limits mobility but reduces the affected person's quality of life.
History

AS has a long history, having been distinguished from rheumatoid arthritis by Galen as early as the second century AD. Skeletal evidence of the disease (ossification of joints and entheses primarily of the axial skeleton, known as "bamboo spine") was found in an archaeological dig that unearthed the skeletal remains of a 5000-yearâ€"old Egyptian mummy with evidence of bamboo spine.
The anatomist and surgeon Realdo Colombo described what could have been the disease in 1559, and the first account of pathologic changes to the skeleton possibly associated with AS was published in 1691 by Bernard Connor. In 1818, Benjamin Brodie became the first physician to document a patient believed to have active AS who also had accompanying iritis.
In 1858, David Tucker published a small booklet which clearly described a patient, Leonard Trask, who suffered from severe spinal deformity subsequent to AS. In 1833, Trask fell from a horse, exacerbating the condition and resulting in severe deformity. Tucker reported:
This account became the first documented case of AS in the United States, owing to its indisputable description of inflammatory disease characteristics of AS and the hallmark of deforming injury in AS.
It was not until the late nineteenth century, however, when the neurophysiologist Vladimir Bekhterev of Russia in 1893, Adolph Strümpell of Germany in 1897, and Pierre Marie of France in 1898 were the first to give adequate descriptions which permitted an accurate diagnosis of AS prior to severe spinal deformity. For this reason, AS is also known as Bekhterev Disease, Bechterew's Disease or Marieâ€"Strümpell Disease.
